VIDEO: Horizontal Canal BPPV (HC-BPPV)- Contraindication to Self Treatment
Published on: October 14, 2014
The incidence of Horizontal Canal (HC) involvement in our 20 years of experience treating almost 11,000 BPPV cases has been its association either with a migration during a CRM treatment, or inadvertently during the patient’s normal everyday activities. Our data (Roberts and Gans, 2008) is consistent with that reported by other investigators with a range of HC occurrence seen on an initial visit (not post CRM) of approximately 10-15%.
Recently however, we have seen almost a three-fold increase in the HC variant during the patient’s initial visit. Why this increase? When asked, at least 70% of the patients report one of three common factors:
- They searched the Internet and found treatments or videos of self-treatments, which they or a family member performed.
- A physician or health care practitioner had provided them with a photocopy of home exercises for them to perform.
- A friend told them how to treat themselves, based on their own past experience with a CRM.
In all scenarios the patient’s self treatment has resulted in an increased severity in the intensity and duration of the vertigo as well as a new bilateral nature. The patient now believes it must be in both ears as they have symptoms when lying on either side. They also may report a sense of dizziness (not true vertigo) with side-to-side head movements and other head positions as well as an increased sense of imbalance. They have gotten much worse, not better.
Argument against self-treatment:
- Cawthorne Cooksey exercises (1946) and Brandt- Daroff (1980) were well intentioned but these articles were written decades before there was a full understanding of the nature of BPPV and its variants and treatments. They were not specific to BPPV and were based on habituation theory. One does not habituate BPPV induced vertigo. This was clearly established with Semont’s article in 1988 followed by Epley and Herdman’s publications in 1992 and 1993 respectively and all those following for the past 20 years. HC-BPPV was not reported in the literature until McClure’s article in 1985.
- Vertigo causes intense spatial disorientation. How can anyone experiencing true vertigo accurately move and maintain their head through a sequence of very specific positions.
- CRM when performed by a capable practitioner is almost 100% successful with one visit (Roberts, Gans and Montaudo, 2006). The CRM therefore is time efficient and cost effective. With virtually no secondary issues other than in those patients with motion intolerance and this may be easily remedied with pre-medication to avoid nausea and emesis.
- Avoidance of doing the patient harm, by promoting them through self-treatment any one of the following: 1.) Horizontal migration, 2.) Tumarkin crisis 3.) Canalith jam 4.) Vertebral artery compromise or dissection
- Why recommend a self-treatment protocol that has an 80% chance of doing harm and only a 20% chance of success.
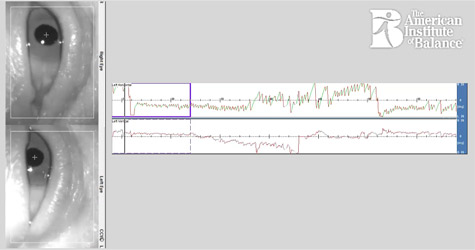
VIDEO – In this video you will see a classic horizontal nystagmus (LBN) produced in a side lying position. In the second part of the video, we demonstrate how to isolate each ear’s respective HC to avoid any migration in patients who may have a positive PC-BPPV.