Vertebral Basilar Insufficiencies (VBI) vs. non-classic BPPV
Published on: February 13, 2013
Current Neurology literature continues to present cases of vertebral basilar insufficiencies (VBI), vertebral artery ischemia (VA stroke) and cervical artery dissections (Choi JH et al, 2011, Kim BM et al 2011, Schievink WI and Debette S, 2011, Volker W et al, 2011).
This should be of particular interest to clinicians examining patients with complaints of positional vertigo; to be sure they are not confused with a “non-classical” BPPV. Many of these patients will have symptoms with hyperextension of the neck with rotation or lateral tilt. Since the condition will be provoked in a static head-neck position, unlike a PC-BPPV, the nystagmus may be of any type (horizontal, vertical or torsional), but most importantly it will not fatigue. Likewise, the patient may report other focal neurological symptoms typically unrelated to a BPPV response. Although there is some controversy as to whether vertebral artery screening is reliable based on concerns of its sensitivity, it is apparent that VBI is a relatively common problem even in young adults. The elderly who have a higher prevalence of BPPV also have co-morbidities of osteoarthritis and cervical spondylosis.
AIB protocol includes:
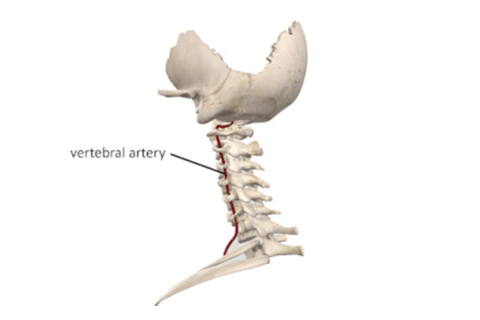
- Vertebral artery screening (VAS) – seated prior to modified Hallpike. Despite the acknowledgement of reduced sensitivity it may provide guidance for selection of testing protocols.
- Modified Hallpike procedures. Fully supported techniques only (no head hanging off table). If the VAS was positive-seated, then only side-lying modified Hallpike will be used.
- If there is no fatiguing of response (i.e. nystagmus, vertigo, nausea), these are likely neuro-vascular symptoms not BPPV.
- A “non” classic BPPV may be seen on occasion without nystagmus, but with a transient vertigo with latency and duration of no more than 10-12 seconds. As reported by Haynes et al. 2002, this may be successfully treated by repositioning and re-checked. If it was a BPPV, transient vertigo should be gone.
- If a VBI is considered, consultation with referring physician and neurology is strongly indicated.
- For those patients with both a VBI and PC-BPPV, Semont or Gans repositioning maneuvers for BPPV treatment are indicated as neither requires hyperextension.