Subdural Hemotoma May Mimic BPPV Post Head Trauma
Published on: June 12, 2013
We see a significant number of patients with BPPV secondary to even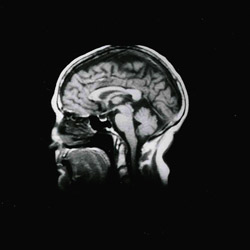 relatively minor head impacts. Falls from bicycles, hitting their heads on night stands, golf carts, car doors etc., that do not force patient to go to ED or seek immediate medical attention. What they consider just a “ bad crack on the head” and the associated headache may not be concerning (they expect a headache after the head bump) until there is an accompanying positional vertigo. Although this is a common occurrence we must be on the alert for more significant injuries.
relatively minor head impacts. Falls from bicycles, hitting their heads on night stands, golf carts, car doors etc., that do not force patient to go to ED or seek immediate medical attention. What they consider just a “ bad crack on the head” and the associated headache may not be concerning (they expect a headache after the head bump) until there is an accompanying positional vertigo. Although this is a common occurrence we must be on the alert for more significant injuries.
Case Study
History: Arising during the night, a 60 year-old male, hit his head on a door while walking in the dark to use the bathroom. Upon awakening the next morning he began to experience an increasingly severe headache and pressure, so he took OTC analgesic and applied ice-packs. By mid afternoon, he had the onset of positional dizziness, most noticeable in a supine position. The following day he was referred to AIB by a walk-in-clinic, for what was suspected to be BPPV.
Findings
· ENT and otoscopic evaluation- unremarkable with no auditory symptoms or otalgia or discharge. Audiologic studies negative for middle ear or asymmetrical SNHL.
· SOP/CTSIB – Abnormal. Unsteady-sway on modified Romberg. Failed dynamic CTSIB with and without vision. Abnormal sway on Fukuda test.
· VNG- Abnormal for a spontaneous low-intensity (4 deg. sec.) downbeat nystagmus (DBN) (vision denied) that enhanced significantly (12 deg. sec.) in positional sub-tests. Modified Hallpike testing was negative for BPPV-PC/HC findings. Ocular motor and caloric testing was unremarkable.
· Rotary Chair and VEMP testing were both unremarkable.
Conclusions
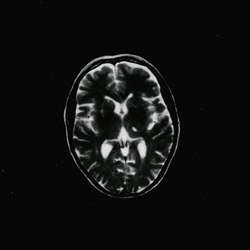
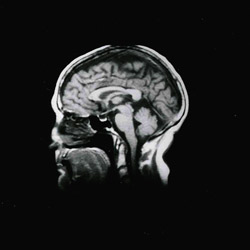
1. Patient did not have BPPV and radiographic studies were ordered based on history, symptoms and presence of the non-transient spontaneous and positionally enhanced DBN.
2. See scans provided showing subdural hemotoma. The patient was referred to neurology for consultation and triage.
3. Patients’ post-head trauma may present with BPPV- unilateral or bilateral, subdural hemotoma or both.