VIDEO – Video Head Impulse Test (VHIT)
Published on: April 8, 2014
Background:
The visualization of corrective saccades as a highly sensitive bedside examination of a peripheral vestibular deficit has been well reported in the literature. The “head thrust” test as described by Halmaygi and Curthyos (1988) and others has shown to be excellent bedside test in revealing status of non-compensated or active labyrinthine conditions including ear specificity. It’s sensitivity and specificity has been reported as high as 100% in cases of total peripheral loss. The direct observation required of bedside testing is however, less sensitive with partial vestibular deficits. The use of scleral coils in the laboratory has provided additional information, but is impractical as a simple office-based procedure.
For those unfamiliar with the test – head impulses are rapid, passive, unpredictable rotations of the head relative to the trunk. With bedside testing, the patient is asked to fix upon a target straight ahead, usually the nose of the examiner, while the examiner turns the patient’s head in the plane of a pair of semicircular canals. The rotations are of low amplitude (10–20°) but of high acceleration (10000°/s2). It is the frequency of the head movement not the degree of excursion, so even patients who may have some restricted range of neck motion (ROM) can be comfortably tested.
If the peripheral vestibular system is intact the vestibulo‐ocular reflex (VOR) operates normally and the patient’s eyes stay fixed on target ( the gaze is held relatively stable in space). If not (due to reduced gain of the VOR towards the side of the head impulse), a reflexive saccade back to the examiner’s nose is observed after the end of the head thrust. This corrective saccade indicates a peripheral vestibular hypofunction on the side towards which the preceding head rotation occurred. The challenge is that this corrective saccade is not always easy to see and is also dependent on a competent tester.
A number of investigators (MacDougall et al, 2009, MacDougall et al, 2013) have reported on a video impulse test that has the same sensitivity as the scleral coils, making it an ideal test for office or bedside. The benefit of course is the higher sensitivity and objectivity utilizing videoculography and computer algorithms.
VIDEO:
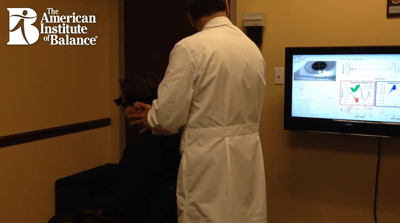
In the video you will see me performing lateral head impulses using an Interacoustics system. There are several manufacturers of VHIT instrumentation, this happens to be a VNG/VHIT combined system. We have the screen displayed on the large wall mounted LCD which gives us very good visualization without straining to watch on a laptop screen. Note that when the technique has been performed accurately and the patient is compliant (meaning they had their eyes focused on the the target) we see a big green check mark when it is a good test and a red X when it is not. So we are not confused trying to analyze poor data. This is a great advantage and also is a great training tool for novice clinicians learning proper technique.
VHIT Clinical Applications at AIB:
- Tests all 6 semicircular canals, unlike other testing limited to only the horizontal canals.
- Tests the VOR at higher frequencies unlike the caloric’s limited ultra-low sensitivity (.003Hz) or even Rotary Chair (.64 Hz). The identification of mid to high frequency active or uncompensated vestibulopathy is of critical importance to an individual’s safety and ability to return to work or daily activities.
- Ideal for individuals who cannot or will not tolerate calorics or when other tests are not readily available.
- Provides an objective measurement of recovery or compensation status to better determine candidacy for vestibular rehabilitation therapy (VRT) as well as the need for specific protocols. This should correlate with tests of dynamic visual acuity. The corrective saccade is the physiological manifestation, which forces the retinal slippage that we term oscillopsia.
- Excellent tool for testing young children who may not tolerate a closed videogoggle.
References:
Halmagyi G M, Curthoys I S. A clinical sign of canal paresis. Arch Neurol 1988. 45737–739.739.
MacDougall HG, Weber KP, McGarvie LA, Halmagyi GM, Curthoys IS., The video head impulse test: diagnostic accuracy in peripheral vestibulopathy. Neurology. 2009 Oct 6;73(14):1134-41.
MacDougall HG, McGarvie LA, Halmagyi GM, Curthoys IS, Weber KP. Application of the video head impulse test to detect vertical semicircular canal dysfunction. Otol Neurotol. 2013 Aug; 34(6):974-9.